The evolution of autism diagnosis is a story of shifting paradigms, where science, society, and stigma have danced in an intricate waltz. From the early whispers of “childhood schizophrenia” to the precise frameworks of the DSM-5, the journey has been as much about understanding the human mind as it is about redefining the boundaries of neurodiversity. What began as a fragmented collection of observations has crystallized into a diagnostic system that seeks to capture the essence of autism—not as a monolithic condition, but as a spectrum of experiences, each as unique as the individual it describes.
At the heart of this transformation lies the Diagnostic and Statistical Manual of Mental Disorders (DSM), a tome that has become both a compass and a lightning rod for clinicians, researchers, and families alike. Its pages have not merely cataloged symptoms; they have shaped perceptions, influenced interventions, and, at times, sparked controversy. To trace the evolution of autism within the DSM is to uncover a narrative of scientific progress, societal awakening, and the relentless pursuit of clarity in a field where ambiguity once reigned supreme.
The DSM’s Early Encounters with Autism: A Fragmented Beginning
The DSM’s initial forays into autism were, in retrospect, more akin to cartographic sketches than detailed maps. In the 1950s and 1960s, autism was a term barely whispered in psychiatric circles, often conflated with schizophrenia or dismissed as a form of childhood psychosis. The DSM-I (1952) and DSM-II (1968) offered scant guidance, describing autism under broad, vague categories like “childhood schizophrenia” or “atypical development.” Clinicians relied on fragmented observations, and diagnoses were as much a product of intuition as they were of structured criteria.
This era was marked by a profound lack of consensus. Autism was seen through the lens of deficit—children who failed to meet developmental milestones were labeled as “emotionally disturbed” or “mentally retarded,” their behaviors pathologized without a deeper understanding of their origins. The absence of clear diagnostic criteria meant that diagnoses were inconsistent, and families often found themselves navigating a labyrinth of misinterpretations. It was a time when autism was shrouded in mystery, its contours ill-defined, and its impact on individuals and families poorly understood.
The DSM-III: A Turning Point in Clarity
The release of the DSM-III in 1980 marked a seismic shift in how autism was conceptualized. For the first time, autism was granted its own diagnostic category, “Infantile Autism,” distinct from schizophrenia. This separation was not merely semantic; it was a recognition that autism was a unique neurodevelopmental condition, not a subset of another disorder. The DSM-III introduced specific criteria, including impairments in social interaction, communication, and restricted or repetitive behaviors, laying the groundwork for future refinements.
Yet, this newfound clarity was not without its limitations. The DSM-III’s criteria were rigid, often excluding individuals who did not fit the mold of “classic” autism. The focus on early-onset symptoms meant that those diagnosed later in life, or those with milder presentations, were frequently overlooked. The manual’s rigidity reflected the era’s broader scientific understanding, which was still grappling with the nuances of neurodevelopment. Clinicians and researchers began to recognize that autism was not a one-size-fits-all condition, but the DSM-III’s framework struggled to accommodate this complexity.

The DSM-IV: Expanding the Spectrum
The DSM-IV, published in 1994, represented a pivotal moment in the evolution of autism diagnosis. It introduced the concept of “autistic disorder” as part of a broader category called “Pervasive Developmental Disorders” (PDD), which included Asperger’s syndrome, Rett’s disorder, Childhood Disintegrative Disorder, and PDD-Not Otherwise Specified (PDD-NOS). This expansion acknowledged that autism was not a single entity but a spectrum of conditions, each with its own nuances.
The DSM-IV’s criteria were more inclusive, recognizing that autism could manifest in diverse ways. The inclusion of Asperger’s syndrome, in particular, highlighted the heterogeneity of the spectrum, capturing individuals with average or above-average intelligence who struggled with social communication but did not exhibit significant language delays. However, the DSM-IV’s structure also sowed the seeds of future debates. The distinction between Asperger’s syndrome and autistic disorder was often arbitrary, leading to diagnostic inconsistencies. Moreover, the “PDD-NOS” category, intended to capture atypical presentations, became a catch-all for cases that did not fit neatly into other diagnoses—a reflection of the manual’s ongoing struggle to balance specificity with inclusivity.
The DSM-5: A Paradigm Shift Toward Unity
The release of the DSM-5 in 2013 marked a radical departure from its predecessors. Gone were the fragmented categories of the DSM-IV; in their place stood a unified diagnosis: Autism Spectrum Disorder (ASD). This change was not merely a semantic shift but a philosophical one. The DSM-5 recognized that autism was a spectrum, and that the distinctions between its various forms were often artificial. By consolidating the diagnosis, the manual sought to capture the full range of autistic experiences, from those with significant support needs to those who thrive with minimal accommodations.
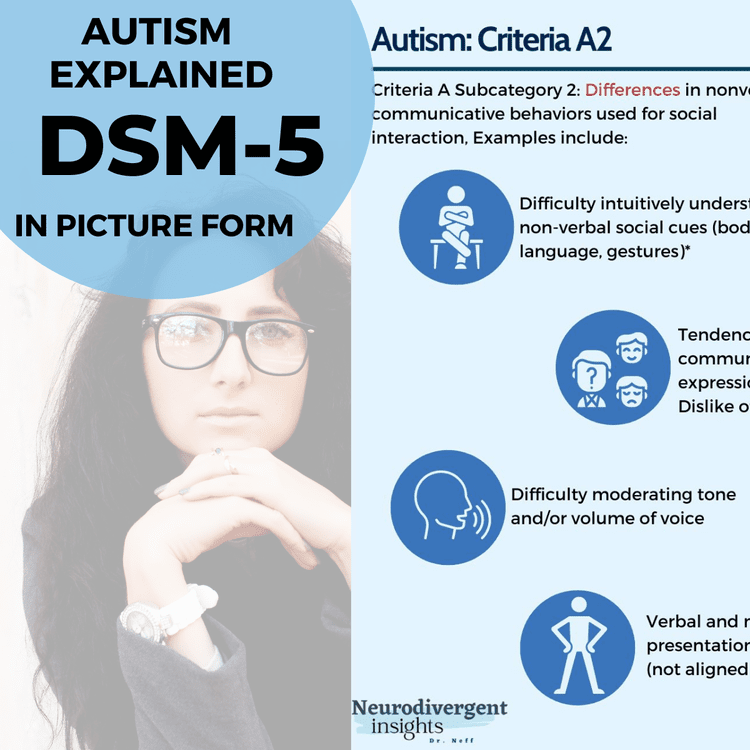
The DSM-5’s criteria emphasized two core domains: social communication and interaction, and restricted, repetitive patterns of behavior. This framework acknowledged that autism was not defined by deficits alone but by a unique way of experiencing the world. The manual also introduced a three-level severity scale, intended to reflect the varying degrees of support required, though this aspect has remained a subject of debate. Critics argue that the levels oversimplify the complexity of individual needs, while proponents praise the DSM-5 for its focus on functional impact rather than rigid symptom checklists.

The Controversies and Criticisms: A Field in Flux
No evolution is without its detractors, and the DSM-5’s changes have been no exception. One of the most contentious issues is the elimination of Asperger’s syndrome as a distinct diagnosis. For many, this was a step backward, erasing the identity of a group of individuals who had long identified with the term. Others argue that the consolidation was necessary to reflect the true spectrum of autism, where the lines between diagnoses were often blurred. The debate underscores a deeper tension: the tension between recognizing individual differences and the need for a unified diagnostic framework.
Another criticism centers on the DSM-5’s reliance on behavioral criteria. While the manual provides a structured approach to diagnosis, it offers little insight into the underlying causes of autism. Some researchers argue that a purely behavioral framework overlooks the biological and genetic factors that contribute to the condition, leaving clinicians without a holistic understanding. This has led to calls for a more nuanced approach, one that incorporates biomarkers or cognitive profiles alongside behavioral observations.
The DSM-5 has also faced scrutiny for its potential to exclude certain populations. The emphasis on early-onset symptoms, for example, may overlook individuals who develop coping mechanisms that mask their autistic traits, only to be diagnosed later in life. Similarly, the manual’s criteria may not fully capture the experiences of autistic individuals from diverse cultural backgrounds, where social norms and communication styles differ significantly from those assumed in the DSM.
The Future of Autism Diagnosis: Beyond the DSM
As the DSM continues to evolve, so too does the conversation around autism. The manual’s limitations have spurred alternative approaches, such as the International Classification of Diseases (ICD), which offers a complementary framework for diagnosis. Research into biomarkers, brain imaging, and genetic testing holds the promise of more objective diagnostic tools, though these are not yet ready for widespread clinical use. Meanwhile, the neurodiversity movement has challenged the very notion of diagnosis, advocating for a shift from pathologizing differences to celebrating them.
The future of autism diagnosis may lie in a hybrid model—one that combines the DSM’s structured criteria with a deeper understanding of individual strengths and challenges. It may involve a greater emphasis on functional assessments, where clinicians evaluate not just symptoms but the impact of those symptoms on daily life. It may also require a more collaborative approach, where autistic individuals and their families play an active role in shaping diagnostic criteria and interventions.
:max_bytes(150000):strip_icc()/What-are-the-three-levels-of-autism-260233-5baab02fc9e77c002c390bd2.png)
The evolution of autism diagnosis is far from over. Each iteration of the DSM has brought us closer to understanding the spectrum, yet each has also revealed new layers of complexity. What began as a quest for clarity has become a testament to the richness of human diversity. Autism is not a puzzle to be solved but a mosaic to be appreciated, each piece contributing to a larger, more vibrant picture. As science advances and societal attitudes shift, the DSM’s role may evolve from a diagnostic tool to a historical artifact—a record of how far we’ve come and how much further we have to go.